| |  |
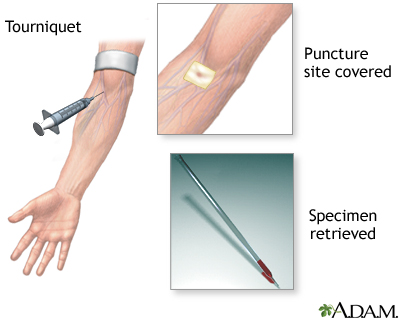
 | |  |  |  |  |  | How the test is performed: Adult or child: Blood is drawn from a vein (venipuncture), usually from the inside of the elbow or the back of the hand. The puncture site is cleaned with antiseptic, and a tourniquet (an elastic band) or blood pressure cuff is placed around the upper arm to apply pressure and restrict blood flow through the vein. This causes veins below the tourniquet to distend (fill with blood). A needle is inserted into the vein, and the blood is collected in an air-tight vial or a syringe. During the procedure, the tourniquet is removed to restore circulation. Once the blood has been collected, the needle is removed, and the puncture site is covered to stop any bleeding. Infant or young child: The area is cleansed with antiseptic and punctured with a sharp needle or a lancet. The blood may be collected in a pipette (small glass tube), on a slide, onto a test strip, or into a small container. Cotton or a bandage may be applied to the puncture site if there is any continued bleeding. How to prepare for the test: Adults: No special preparation is necessary. Infants and children: The physical and psychological preparation you can provide for this or any test or procedure depends on your child's age, interests, previous experience, and level of trust. For specific information regarding how you can prepare your child, see the following topics as they correspond to your child's age: infant test or procedure preparation (birth to 1 year) toddler test or procedure preparation (1 to 3 years) preschooler test or procedure preparation (3 to 6 years) schoolage test or procedure preparation (6 to 12 years) adolescent test or procedure preparation (12 to 18 years) How the test will feel: When the needle is inserted to draw blood, some people feel moderate pain, while others feel only a prick or stinging sensation. Afterward, there may be some throbbing. What the risks are: Risks associated with venipuncture are slight: excessive bleeding fainting or feeling lightheaded hematoma (blood accumulating under the skin) infection (a slight risk any time the skin is broken) multiple punctures to locate veins Veins and arteries vary in size from one patient to another and from one side of the body to the other. Obtaining a blood sample from some people may be more difficult than from others.
|  |  |  |  |
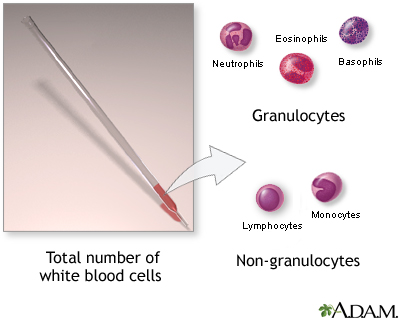
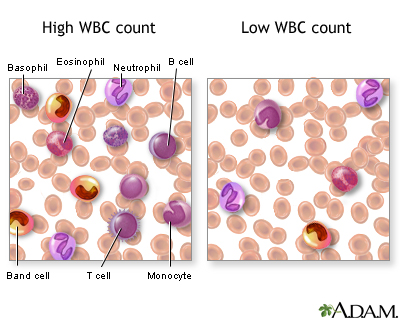
| | | | | | | Interfering factors: Acute emotional or physical stress can increase WBC counts. There are various types of white blood cells (WBCs) that normally appear in the blood: neutrophils (polymorphonuclear leukocytes; PMNs), band cells (slightly immature neutrophils), T-type lymphocytes (T cells), B-type lymphocytes (B cells), monocytes, eosinophils, and basophils. T and B-type lymphocytes are indistinguishable from each other in a normal slide preparation. Any infection or acute stress will result in an increased production of WBCs. This usually entails increased numbers of cells and an increase in the percentage of immature cells (mainly band zcells) in the blood. This change is referred to as a "shift to the left" People who have had a splenectomy have a persistent mild elevation of WBCs. Drugs that may increase WBC counts include epinephrine, allopurinol, aspirin, chloroform, heparin, quinine, corticosteroids, and triamterene. Drugs that may decrease WBC counts include antibiotics, anticonvulsants, antihistamine, antithyroid drugs, arsenicals, barbiturates, chemotherapeutic agents, diuretics and sulfonamides. Normal values: WBC: 4,500 to 10,000 cells/mcl Note: cells/mcl = cells per microliter What abnormal results mean: Low numbers of WBCs (leukopenia) may indicate: bone marrow failure (for example, due to granuloma, tumor, fibrosis) presence of cytotoxic substance collagen-vascular diseases (such as lupus erythematosus) disease of the liver or spleen radiation High numbers of WBCs (leukocytosis) may indicate: infectious diseases inflammatory disease (such as rheumatoid arthritis or allergy) leukemia severe emotional or physical stress tissue damage (for example, burns)
| | | | |
|
Review Date:
2/13/2011
Reviewed By:
David C. Dugdale, III, MD, Professor of Medicine, Division of General Medicine, Department of Medicine, University of Washington School of Medicine. Also reviewed by David Zieve, MD, MHA, Medical Director, A.D.A.M., Inc. The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Call 911 for all medical emergencies. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. © 1997-
A.D.A.M., Inc. Any duplication or distribution of the information contained herein is strictly prohibited. | © 1997-

All rights reserved.
|
|