Gastroesophageal reflux
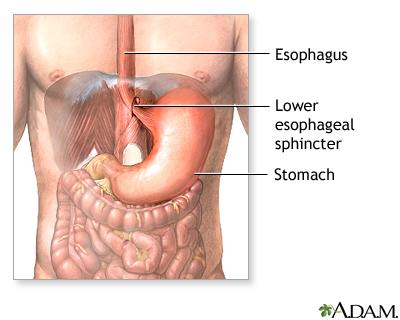
| Normal anatomy |
The esophagus is a narrow, muscular tube that carries food from the mouth to the stomach. A muscular ring (sphincter) at the junction of the esophagus and the stomach prevents reflux (backflow) of food and acid from the stomach into the esophagus.
|
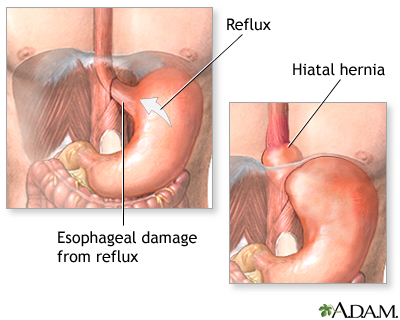
| Indication |
When the lower esophageal sphincter doesn't function properly, acid and food can reflux up from the stomach into the esophagus. This can lead to pain (heartburn) and damage to the lower esophagus. Over time, this damage can sometimes produce strictures (narrowing) of the esophagus and may even lead to cancer of the esophagus. Frequently, dysfunction of the lower esophageal sphincter is associated with a hiatal hernia, in which the upper part of the stomach slips up into the chest.
|
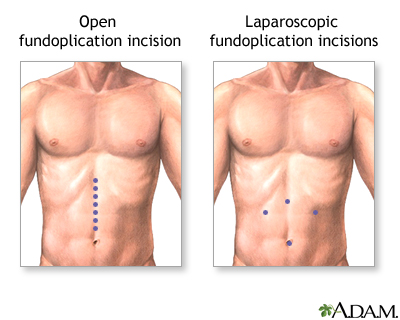
| Incision |
The first step in managing esophageal reflux disease involves medical treatment. Lifestyle changes (diet, smoking cessation, sleeping position) should always be the first step. Antacid medications can neutralize acid that refluxes into the esophagus and prevent damage to the esophagus. More effective medications can sharply reduce the production of acid. If these medications do not eliminate symptoms, surgery may be necessary. The primary surgical treatment of esophageal reflux is called esophageal fundoplication. Fundoplication can be performed through an upper midline incision or using a laparoscopic procedure.
|
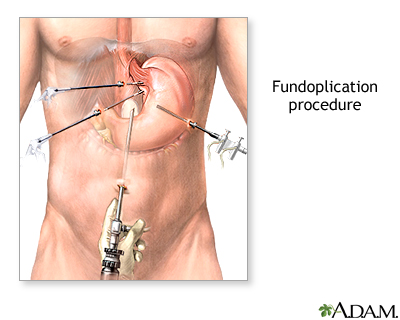
| Procedure, part 1 |
The laparoscopic procedure is being performed more frequently. Long narrow instruments are passed through small incisions in the abdomen. The surgery is viewed through a long narrow fiberoptic tube passed through one of these incisions.
|
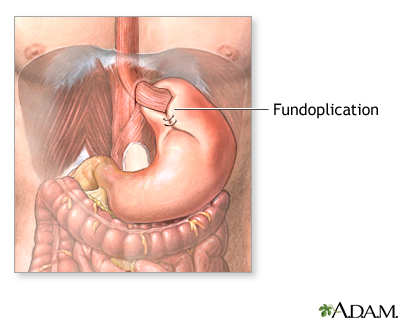
| Procedure, part 2 |
There are a number of different types of fundoplication procedures, which all involve wrapping a part of the upper stomach around the esophagus and reinforcing the lower esophageal sphincter. The most commonly performed fundoplication procedure is called Nissen fundoplication. Fundoplication generally has excellent results and cures reflux disease without the need for lifelong antacid medications.
|

|
Review Date:
12/22/2011
Reviewed By:
Harvey Simon, MD, Editor-in-Chief, Associate Professor of Medicine, Harvard Medical School; Senior Physician, Massachusetts General Hospital. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. © 1997-
A.D.A.M., Inc. Any duplication or distribution of the information contained herein is strictly prohibited.